Even though lung cancer is one of the most common cancers in the United States, many people are unaware of its reach and impact. Did you know, for example, that lung cancer is the No. 1 cancer killer of women, according to the American Lung Association? Over the past 37 years, the rate of new lung cancer cases has nearly doubled in women, and yet only 1 percent of women have the disease on their radar.
The American Cancer Society estimates that 228,150 new cases will be diagnosed in 2019— 116,440 in men and 111,710 in women. Although cigarette smoking is an important factor, 28,000 Americans living with lung cancer have never smoked, the American Lung Association reported.
But there’s good news. Today, thanks in large part to improvements in diagnostics and treatments, thousands of people are surviving lung cancer. The key is to catch it early, when the survival rate is much higher. Still, most cases are not diagnosed until advanced stages, which makes awareness initiatives around early detection efforts all the more important.
One medical advance that is offering oncologists new tools in the fight against lung cancer is immunotherapy. It uses the body’s own immune system to detect and fight cancer cells. “Tumors have ways of protecting themselves and ways to get around the body’s natural defenses to attack what’s not normal,” says Kendal Hervert, DO, FCCP, Pulmonologist at our Tulsa hospital. “These therapies are finding a way to shut down those defenses.”
Checkpoint inhibitors like pembrolizumab (Keytruda®), which President Jimmy Carter took to treat the metastatic melanoma that spread to his liver and brain, work by tricking the body into doing what it was designed to do. Think of cancer cells as biological double agents. They are the body’s own cells that have mutated and turned against their host. But because they are not foreign, they often sneak past the immune system’s defenses. These double agents have a way of sending deceptive signals to antigen-fighting T-cells that they are not harmful. “Nothing to see here,” they wink to T-cells that pass through various checkpoints in search of invaders. If not for these checkpoints, T-cells would run amok and hunt down healthy cells. But immunotherapy is designed to turn those checkpoints off and disrupt the cancer cells’ signal, exposing them and unleashing the immune system to attack.
“Cancer is like a wolf in sheep’s clothing,” says Eugene Ahn, MD, Medical Oncologist at our Chicago hospital. “The body perceives it as a member of the flock. These medicines help remove the sheep’s clothing.” Other forms of cancer immunotherapy have been used over the years, and still more are being developed.
Another development involves the use of targeted therapy, which blocks cancer’s growth by stopping cancer cells from dividing or by killing them directly. “Targeted therapies allow people to continue on with their daily lives because they don’t have to go in for chemotherapy infusions every two or three weeks,” Hervert says. “Typically, it’s a pill that they take on a daily basis, and it allows them to feel a little bit more like they’re just having their routine.”
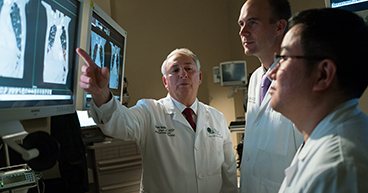
Other improvements have been made in the area of diagnostics. For example, expedited diagnostic programs, like the one now being offered at our Chicago hospital, can cut down considerably on the amount of time patients have to wait for test results. With the hospitals’ rapid lung-nodule diagnostic program, a medical team—consisting of a medical oncologist, an interventional radiologist, a pulmonologist and a thoracic surgeon all working together under one roof—reviews relevant scans and records before the patient comes in. If more images are needed, a biopsy is performed that day and immediately examined by a pathologist. By day four, the medical team shares the diagnosis and, if cancer is found, recommends a personalized treatment plan specific to the patient’s needs.
“We think it will improve quality of care if an early diagnosis is done efficiently, and it will improve the emotional and psychological stressors that go with knowing ‘something’s wrong, and I don’t have a treatment plan,’” says Bruce Gershenhorn, DO, Medical Oncologist at our Chicago hospital.